Greetings Everyone, and thank you for coming.
Kyle James
Born: March 6th 2004 12:39 AM CST - 5' 9 Oz - 20.5 inches long
Died: March 25th 2004 1:45 PM CST
13140 181st Drive NW - Elk River, MN 55330 (763 274 0994)
- jim@yothers.com
Funeral Information
All are welcome to come
Monday March 29th 2004
Central Lutheran Church in Elk River
Viewing 1:00 PM
Service 2:00 PM
Following the service there will be a processional to the grave site over looking Lake Orono in Elk River
Following completion of burial will be a luncheon back at the Church.
Funeral Direction provided by:
Dare's Funeral Service 805 Main Street,
Elk River, Minnesota 55330
(763) 441
1212
March 25th morning (before
sugery) |
|||
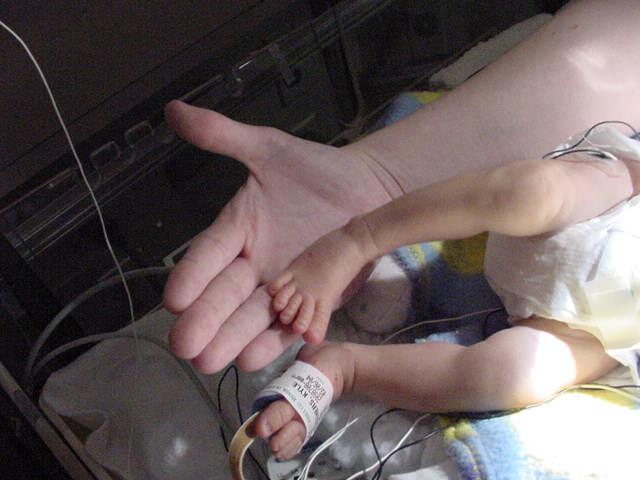
March 25th afternoon (passing
away) |
|||
March 25th 2004
Kyle went into surgery today with fairly high hopes. The bruising on his arms had increased significantly overnight. The surgery went well and the shunt placement was working good. When the surgeons pulled back the drapes from the rest of his body (which they cover everything except where they are working) they found that the bruising on his arms traveled further up and had become very purple in just the couple hours in surgery. We already knew we was going to lose finger tips, and possibly his hands. Now with it traveling and having no idea why it will encompass his entire body within the day. It was explained to us (which we already figured) was that it was a snowball effect. The body puts off chemicals as parts of the tissues die. His finger tips had already begun to shrivel, and were completely black. Much like frostbite. This effect now was going to take over his entire body. To combat this issue would undo everything we just did to his heart over the past week. There was nothing anyone can do. The end is inevitable.
Rachel and I both went to a secluded room, they disconnected all the wires, all the tubes, and we got to hold him in our arms. He was still under drugs from surgery so he felt no pain. They turned off the machines, and at 1:45pm CST he died in our arms.
I will get any funeral arrangements that are made to this page if any one is interested. Please do not call. Send an email if you would like to say anything to us. Thank you to everyone for your prayers, to the people at the hospital with their incredible skill and warmth, it just wasn't enough.
It has been a tremendous joy, and a crushing tragedy depending upon which time you talked to either Rachel or myself. So instead of each person getting to hear our emotions of the time (as they can tend to fluctuate rapidly) I am putting the web page together so anyone can get the latest information we currently have. The latest news will always be at the top. At some point I will thank everyone for all their wonderful heart felt support through all this, in the mean time please accept my gratitude, and know that your support continues to fan the flames of our love for our son. - PS I apologize for any spelling mistakes before hand.
March 24rd 2004 - So today we go to see Kyle with a heavy heart. It was a very quiet drive to the hospital for both Rachel and I. Last night was grueling, but we had each other. We arrive and told once again that the head unit will need to be changed. We look at his hands and feet, and the hands look terrible. His finger tips are basically black with lighter shades of red going back up his arms. His feet seem to look better, there is still a dusting of purple on his left set of toes. Dr Wright (Whom we have discovered is a very optimistic person) and he has informed us of the positives that Kyle has gone through the night and he is impressed. Kyle lost a lot of weight (fluids) and urine output is great. As of this morning his coagulants (clotting agents in the blood) are stabilized. He did show concern for Kyle's hands but refused to say that they will be lost. Tips likely, but not the whole hand. He cannot explain why his hands are doing what they are doing, and that this was the first time in a cardiac scenario that he has seen this occur. Usually this occurs with infection patients.
We then spent time with Kyle letting him know we loved him, and that there was nothing we wouldn't do for him. We let him know of everyone's prayers and the emails that I receive, even from the unknown people that I get them from. We then stepped out while they changed the head unit on the ECMO.
Once we stepped back in, Dr Moga was there (Whom we discovered now to be very pessimistic). He too stated he was impressed by Kyle's rebound from yesterday. They have tentatively scheduled surgery for 8:30am thursday morning. If he doesn't crash like he did the previous night then it should be a go. He will be putting the shunt in place, and replacing the ECMO for a version that allows cutting down the flow. This will be another 4 hour operation. He will be coming out on an ECMO, but one we can wean him off of. He mentioned Kyle's hands and said that the damage to his hands had been done, and there is nothing they can do to stop it. They are not sure why it is happening, and had they known they would have gone way out of their way to prevent or avoid it. He said it looks as though there is a high probability that he will lose his left hand, defiantly the finger tips on both as they are becoming black. The left hand seems to be worse than the right hand. He says he has to play off what Kyle wants to do. If he keeps coming back then do the surgery and proceed from there. If he slides back again, then we make decisions then. He restated that they will go in tomorrow morning, and take a look. It is not so much that the procedure will take a long time, it is more watching what Kyle wants to do. His heart sounds (Wave pattern) looks much better, and as if his heart wants to continue. He said that Kyle defiantly was not making this easy at all. And even after the surgery we are still not out of the woods yet. This is a minor step in the whole process, but at least at this point some definite decisions will be able to be made. Both Rachel and I are tired of all the generic summarizations and shrug of the shoulders and waiting. But we do what we gotta do.
March 23rd 2004 - Kyle's swelling has gone down considerably and his urine output is double what they are putting in. His arterial line (IV straight into an artery) that checks his blood pressure and supplies medicines stopped working this morning. They have been trying all day and in all locations to get it reconnected. His extremities (hands and feet) are getting worse. The bruising is growing up the extremities. The circulation is very marginal. As of 5pm today they still have not been able to get the line reconnected. We talked with his surgeon and received the worst news about his condition. His hands and feet are indicators that he would not survive a 2nd surgery. His blood clotting chemicals within him are not good. The 2nd surgery would be to close up his chest (yes it is still open) and start decreasing the amount of effort provided by the bypass machine. Our week time frame ends on friday for life expectancy on the bypass. Without writing down exactly what is going on, I will let you put 2 and 2 together. We are back to hour by hour for any hope to come in, but right now it doesn't look to hopeful.
March 22th 2004 - His swelling has subsided a bit. Nothing drastic but we can see a little less around his face. The staff was delighted to see his urine output had increased and he was now outputting more than they were putting in. The surgeon had remarked that he was much more optimistic at this point. His abdomen had become softer and his liver was now relaxed. Still puffy, but progressing. They decided not to do surgery today or tomorrow, likely they will wait till Wednesday. We still want the kidney function to increase. We watched today and he was going really well. In lue of time constraints they may do the dialysis to get the swelling down so he can go into surgery as it is important that he come off the ECMO (bypass) as quickly as he can. The pooling in his hands is still there. It looks slightly worse, and the surgeon is still concerned. Again today the bypass machine needed pieces replaced. It took them only 1 min today.
On a personal note we still have difficulty seeing our son like this. None of this is easy for anyone involved. Rachel and I both have become very numb to emotions at this point. As much as we may seem cool and collected, we are very scared and full of emotions. We are asked "How can you do this?" or "How do you keep it together?". The easiest answer is this - Because we have too. Our love for Kyle keeps us going to him day after day. We have coast to coast prayer chains asking the Father to help Kyle, and to help us. This may be well of strength offered to us to wake up each day and see our son in such a condition, and set aside the pain of revelation of possibilities he has to face every hour of every day. There are times we cannot ignore everything attached to him and we break down. Rachel and I have each other for support, and strength in the knowledge that our daughter Kjerste is taken care of.
Thank You to everyone for everything.
March 21th 2004 - We arrived at the hospital and found that Kyle was swollen a bit more. He had stabilized and according to the doctors his urine output was matching as much as they were putting in. He needed to put out more than they were putting in to get the swelling down. If he did not start doing better on that he would have to be put on a kidney dialysis machine. His puffy little hands were showing signs of blood pooling. The doctor was concerned about this. If it gets too bad he could lose his hands. They decided to thin his blood a little, and increase the pressure on the bypass machine to try and prevent the loss of his hands. The bypass machine was getting clogged up with old blood and needs to have parts replaced with fresh ones. This is an expected process and the talented staff that holds vigil over him do an amazing job. As scary as it is, he was off bypass a total of 1.5 mins. He recovered perfectly.
March 20th 2004 - 4pm - We returned to the hospital with much less stink to us, and looked much better. Kyle to looked much better. They did clean him up and covered some tubes up a bit. His kidney function did pickup more. He is still stable. We did take pictures of it. The link following this paragraph will take you there. All his blood work is coming back well. The surgeon did say he was optimistic, and that Kyle was coming along well. Tomorrow is still another story but we are taking everything one moment at a time.
Click here for 3/20/2004 pictures
March 20th 2004 - 8am - We awoke this morning and found Kyle had made it through the night. We were able to rest because the nurses would have come to us had there been any problems. The surgeon had called almost every hour over night, and came in every 3 hours to change his dressing. The dressing would look like someone put a big piece of raw beef on his chest over a period of time. We arrived right when they were finishing up a new dressing. And were able to talk to Dr Moga right away. As of 4am this morning they did not have to give volume to his system to sustain his blood pressure. So he was well on his way to stabilization. His kidney function picked back up. He was not producing as much as they would like to see, so they will give him a dierrietic to help clean out his body. This will help with the puffiness and help the drainage. There was some fluid buildup in the right side of his chest, so they put ANOTHER drainage tube in him. The original 2 had become much clearer, with very little in them to drain. They planned on doing an ultrasound on his head to make sure he was not hemoraging, and they were going to X-ray his chest to make sure everything was still doing well. Dr Moga stated he was now optimistic, with a little concern, but was glad to see Kyle stabilize. We are not out of the woods yet, and to keep with that metaphor we are just getting to the point that we might know where we are and pick a direction.
So with the news being much better than it was the night before, Rachel and I headed home to clean up, grab some food, see our daughter, make an overnight back (just in case) then head back to the hospital.
March 19th 2004 - (DAY OF SURGURY) - (5 pounds 15 ounces) - Rachel and I arrived at the hospital at 7:30am. We immediately went to Kyle, and were able to hold him, touch him, talk to him, and let him know we loved him. Everything was being prepared all around us. Nurses were hovering, and moving furniture and equipment. They moved the warming bed that he had been on out, as he was now going to be on an adult size bed for surgery. The cardiologist that has been with Kyle from day one stopped by and talked a little about what we should expect. We talked about all the possibilities, and that the surgeon performing the operation would be in to talk to us about all this before going into the operation room. We then stepped out for the final prep work of Kyle.
We came back into the PICU to see that Kyle had been venilated (put on a lung machine) and has been sedated. Kyle's surgeon is Doctor Frank Moga. Very young (looking) and very smart. He explained that once again they had taken a view of his ECG with all the attending cardiologists. At this point they were concerned about 3 things, and were going to take steps to take care of these 3 things. The idea was to get Kyle stable, and send him home. This would allow him to grow, get some weight on him, and get him out of the hospital environment. These 3 things are:
1. DSK (Using a shunt (TUBE) connect the pulmonary arteries (arteries to the lungs) to the Aorta)
2. Attaching the Aorta to the Left Ventricle (The correct placement for it), closing off the pulmonary artery from the heart and attach it to the Aorta (providing 2 paths of flow to the Aorta)
3. The pulmonary arteries and veins (to and from his lungs) appear to be too small. They will require enlargement.
At 10:30 am we walked with Kyle to the OR as far as we could go, gave him kisses, and let him know we love him. It was incredibly difficult, extremely scary, and deeply painful to watch him go. We were then escorted to the surgical waiting area where we were giving a pager (incase we needed to be contact by the surgical staff) and they gave us our own waiting room. Bob and Sharon stood watch with us while we waited. My parents were due down at the hospital in the afternoon. We didn't want too many people hanging out with us too long during the dull drum as it would have raised our anxiety.
At 3pm the attending doctor came out and gave Rachel and I an update. He described in some detail about the process and how it was going. He was also periodically letting us know when major steps had gone through the surgery. He let us know that the planned 3 steps had taken place and seem to go very well. They ran into a problem while they were bringing his heart back online (off the bypass machine). There are arteries that attach to the Aorta that feed the heart muscle itself. During the transition back onto his heart, one of these coronary arteries did not fill backup as expected. The right side of his heart was back to original, but the left side was not beating enough to support life. This is the side we are expecting to do 1 1/2 times its normal load due to the right side being too small. This is not a good sign. They immediately reversed gears, put his heart back on ice (this causes the muscle to stop pumping) and back on the bypass. It was explained to us that the first 2 hours the surgeons had to spend on just figuring out were everything went on his heart. There are numerous anomalies in his heart. The attending doctor then wanted us to know that they were in the process of cutting back in to find the problem. And once the problem was found try to discover a solution.
At 4pm the attending doctor came back and let us know they found why it did not pump correctly. The coronary artery seemed to have been torqued/twisted/pinched from the move of the Aorta to the correct placement on his heart. His heart does not want to work quite right, and they attempted to bring him off bypass. Although there was improvement from before, the heart had been worked while not getting enough blood. He would have to be put on an ECMO (portable bypass machine). They could not complete the operation due to having to leave the plumbing in place for the ECMO to work.
At 4:30pm the surgeon Dr Moga came in a talked with us about the surgery. He explained about the coronary artery for the left side of his heart and how it normally would be attached to the Aorta in a normal heart. Kyle's attached very high, and twisted around to the wrong side. This left him with a 1mm place to get things moved. And within that 1mm was just not enough to get things in the right place it seems. He was able to get the coronary artery loose enough to regain appropriate flow and have to watch to make sure it stays that way. He exclaimed how the rest of the procedure when brilliantly until this problem arose. He said he didn't like the way things were, and was very unhappy to have to describe this. He was worried. In the current situation, the left side did not pump well enough to supply life. He will have to remain on the bypass until they can get the heart beating as it should. He can only remain on the bypass for a week. If they cannot get the heart beating on its own by then we have to talk of other alternatives. Also the longer he remains on the lung machine he gets higher and higher chances of scaring his lungs. The plan for tonight is to get him stabilized, and get the kidney function back (pee). Kyle was available to us in the PICU for us to see. He warned us of how he is going to look. They do not close the chest after surgery as they expect the heart to swell (as well as the rest of the body), and it needs a place to swell too. Also they will have drainage tubes from his chest. And in addition to all 7 IV pumps, and 5 Syringe pumps all going into his body, he will be on the bypass that takes the blue blood (non-oxyginated) from the body, gives it oxygen, and returns it back to his body. They are not sending any blood to the lungs to get oxygenated. These tubes are much bigger than the drainage tubes.
There is absolutely NOTHING that can prepare you for the site of seeing your child connected to so many machines, and tubes. Rachel and I both broke down, and came very close to having to walk right back out. As numb as we had become over the last weeks emotions almost overwhelmed us. There was no life in him. He was sedated because of the lungs, and bypass. Blood traces can be seen everywhere. A large gauze bandage over his entire chest was saturated with blood, all the drainage tubes were full of blood, the huge bypass tubes were engorged with blood, and syringes of blood lay everywhere as the nurses remained pushing blood into his small tiny body. He kept losing pressure and they had to keep introducing volume (blood and blood products) to keep it where is should be. This is what the surgeon wanted to become stable. Our emotions, senses, feelings, thoughts are off in left field at this point. There is no reasoning, or rationality that can come to us, to pull us from the deepest pit of despair we have ever felt in our lives. Everyone including the surgeon, nurses, doctors, and us were scared. We were all hopeful and praying, but worried. I personally could only be in there for so long before my mind would get the better of me and I had to stop looking. The fingers we once touched and the hands we once held remained cold, and lifeless. Everything at this time seemed very bleak.
We were so very torn between staying with Kyle, and going home to Kjerste. Nothing had gone to plan today. The hospital informed us that they reserved a sleeping room for us for the night. We arranged for Bob and Sharon to let Kjerste spend the night, and we kissed and hugged my parents off, and we retreated to the sleeping room so Rachel could finally pump. We said good night to Kyle, and told him we will see him in the morning and he better be there and we finally went to sleep around 1am.
March 18th 2004 - For the past 4 days Kyle has been getting stronger. The lack of updates had been due to drawing a new picture of what the surgeons were going to do to him. I have been trying to logically explain what is going to happen. The doctors have been VERY good in dealing with our questions.
Click here for the updated heart picture
March 13th 2004 - Belliruben (Jaundice) has cleared up and the count is now 10.25. They have removed him from the lights, so I was able to get some pictures with his eyes actually open!!! YEAY!! He has more strength now, and stays awake longer and can nurse more. Although today when we tried he got next to mom and decided it was sleepy time. Enjoy the pics though. I apologies for not updating the last 2 days. Kjerste has started to act out and we are trying to spend as much time as we can with her too. We are receiving a lot of notes of prayers, worry, excitement, sadness, and blessings. They are greatly appreciated!! Many ask us what they can do for us, and currently as of today is basically food!! With both Rachel and I not coming home until late in the evening we end up eating around 11pm. Anything that we can freeze then heat up in the microwave would be perfect. Especially if it is something a 6 year old would eat. Besides that all the love and support is stupendous and we do hear your prayers. Kyle looks too good to be in a hospital. Thank you!
March 12th 2004 - No Change - Oxygen is still averaging 90%. He was able to nurse from mom for 10 minutes, of which 5 minutes were latch and suck!!
March 11th 2004 - Oxygen is still averaging 90%, slight eating problems but we are told that is expected. Rash from Bellieruben (Jaundice)
March 10th 2004 - His oxygen level is now definitely decreasing and his heartbeat is changing to compensate. The connecting blood vessel must be closing more. Kyle is slated for another ECG this friday to get an idea of how he will be before the weekend. The 02 stats are now hovering around 90%. He has gained weight although the doctors seem to think it maybe water weight, but I think he has just started to fill in his skin. His IV started to swell in his right arm, so they had to take it back out and put it back on his head (poor guy). Otherwise he is the same. The nurses are now becoming very aggressive about having mom's milk, and have asked Rachel to go to an even higher gear (poor gal). Can you say tender?!
So with surgery eminent, and it looks like the prostaglandin will be as well, I took more pictures before he gets put on the respirator.
The eye cover is for protecting his eyes while they shine a light on him. It is due to him being slightly Jaundice
March 9th 2004 - Kyle's health remains stable. Doctors are very please. After the ultrasound they were able to determine that the connecting blood vessel has indeed started to close. Sunday morning it measured 4mm and this morning it has measured 3mm. His oxygen level remains high, which is good. There are times that it descends to the lower 90s but that is still very well and good. There was some issues with their network servers so they had a bit of an issue getting everything together so the doctor group could gather their thoughts together as a group on the possible directions to take with Kyle. Turns out that Kyle is a picky eater. Go figure, my child a picky eater... His stomach will only digest breast milk. When the nurses put formula in his belly it sits there until she comes back, but if she puts the breast milk in, he empties his stomach, and begins to cry when its empty. YEAY!! So once again, mom and dad are working to get the milk production in high gear. The doctor came back that afternoon and told us that they decided on a plan. The server had come back up and he was able to round them all into looking at it all at the same time. Because his right ventricle is so small, they only feel comfortable allowing it to pump for 1/2 his body. So they cannot to the complete switch. So to my best ability here is the process they will take. I am still unsure if this is more than 1 surgery. It will be scheduled for the next week Wed through Friday is the window.
1. Connect the Aorta to the left Ventricle
2. If the connecting blood vessel is still open, surgically close it, and put a shunt in.
3. Connect the right ventricle to the Pulmonary Artery via the jugular.
March 8th 2004 - Go to the hospital first thing in the morning, and missed the doctor before he leaves the hospital. We review the notes with the nurse. They are not going to do the ECG today and the doctor is very please to find Kyle very stable at the moment. They would like to start feeding him again (so mom needs to do extra pumping) to make sure he gets exactly what he needs and fatten him up. If he can eat and get stronger while staying stable the better off he will be when it comes to surgery. ECG is scheduled for the next day, to confirm the findings on the first ECG, and do more discovery. The doctor is scheduled to be in the hospital all day tomorrow so we should be able to have a private conversation with him at that time. Leave the hospital at 5pm to go pickup Kjerste from day car. Still no Kyle :(
March 7th 2004 - 9pm - Leave the hospital and go home :(
March 7th 2004 - 3pm - After some seriously emotional hours we get ourselves together while at the Children's hospital and review everything with the nurses and care takers there who have gone over everything with the cardiologist. At this time Kyle is very stable. So much so he doesn't need any help breathing, or with oxygen, or any other part of his system. He dirties his diapers, cry's, eats, stays warm, and has plenty of oxygen while he is resting. As soon as he moves or starts crying the saturation of oxygen in his blood goes way down. We are reminded constantly that these problems are fixable. The confidence in the staff there is very reassuring. They are going to stay in a waiting phase as the PDA will be closing off (as it does normally in all new borns) within the next 3-5 days. They will need to know if he can sustain an acceptable amount of oxygen in his blood if it or while it is closing. If he cannot sustain and acceptable amount, they will administer Prostaglandin. A drug used specifically to keep that blood vessel open. Although once administered he will need to be ventilated as the side effect is poor breathing. Right now he is stable while it is open, and if they need to keep it open to keep him stable they will do it.
March 7th 2004 - Noon - Discharged from Mercy hospital. We run home to take care of our now confused, anxious, and upset 6 year old because Kyle did not come home with us. We get cleaned up, give hugs and kisses, then head down to Children's hospital which Kyle was EVACd to.
March 7th 2004 - 11am - Doctor and technician do the ECG on Kyle with Rachel and I watching. We are taken to another private room and describe in some detail the 3 issues Kyle is facing. 1-His greater arteries are reversed. (Click on this link for a REALLY GOOD description of what this is) 2-He has a hole between the lower ventricles (which is a side effect of issue 1). 3-The right ventricle (the only chamber that pumps blood out to your body) is too small to support life. The PDA (an artery that connects the greater arteries (connected blood vessel) while in the womb because as the lungs are not inflated there is no need to send all the blood that way) and the hole in the lower ventricles supply enough oxygenated blood (mixed) to the rest of his system to basically keep him healthy. With only a slight exertions though it feels like your breathing at 10K feet which makes him tired. (Click this link for a picture of exactly what his heart looks like) This explains his problem feeding. The suck works great, it is just that he gets tired very quickly and must rest. Too much oxygen is used while sucking.
March 7th 2004 - 8am - Informed a heart specialist is scheduled to come up with technician to do an ECG (Echo Cardio Gram (Ultra Sound)) on Kyle's heart.
March 7th 2004 - 6am - The float nurse is back in and discussing having the Children's specialist come up and review Kyle. There hasn't been improvement, and he needs to stay in level 2.
March 7th 2004 - 2am - The nurse comes into the room and talks with Rachel (whom let me sleep). She informs Rachel that Kyle is being admitted into the level 2 nursery as he is having a bit of a problem eating, and the breathing is slightly off, the murmur is strange, and he is colder than he should be.
March 6th 2004 - 8pm on - We finally get back to business with Kyle and we have been having a bit of a problem getting him to eat all day. It is not so much to worry about with new borns, but because he is under weight and is expect to lose some weight it is best to make sure we can get him eating as soon as possible. With all the bustle going on around us, and no privacy there was not much we could do. We could not get him to take the breast as he would suck 2-4 times then go to sleep. The doctors had mentioned he had a slight heart murmur in the begriming, and being so little, and slightly early he may not have his suck in order yet. When the float nurse for the night that comes in who hails from the Children's Hospital in Minneapolis comes on she has a bit more concern over the entire thing. She asks that after the midnight feeding that we bring him to the nursery for his routine 24 hour checkup which will take some time. Mom and dad being so worn and smelly at this point take an opportunity to clean, change, and grab a cat nap.
March 6th 2004 - 8am -> 8pm - Visitors and phone calls basically non-stop - Finally we got pictures of Kyle.
March 6th 2004 - 4:00am -> 8:00am - clean recouped drugs for mom and baby
March 6th 2004 - 3:30am - We walk Kyle to our boarding room.
March 6th 2004 - 1:00am - The placenta is passed.
March 6th 2004 - 12:39am - Kyle James is born after 3 pushes.
March 6th - 12:30am - Anesthesiologist administers a test dose. Rachel exclaims she has to push, and can't stop it. They lay her back and check, and she has become fully dilated and inform her that if she wants to push to go ahead.
March 6th 2004 - 12:15am - Anesthesiologist has arrived and starts prepping for the epidermal. Through incredible contractions Rachel must hold still while she receives her epidermal.
March 6th 2004 - Midnight - Pain is definitely unbearable, and the Anesthesiologist is no where to be found. Rachel feels a great burden to pass her bowls as Kyle is now descending.
March 5th 2004 - 11:30pm - Nubain has worn off and she is now definitely in active labor and headed towards transition. Contractions are very painful and breathing through them is not working anymore. Rachel discusses with the nurse and orders an epidermal. Nurse checks her, and now she is at a 6-7.
March 5th 2004 - 9pm - Labor is now a little to painful to deal with. Measuring 3 Rachel elected to be given NuBain as a pain killer to take the edge off the contractions. It worked great! Made her feel slightly drunk and allowed her to sleep. It only last for 2 hours though.
March 5th 2004 - 7pm - Labor pains are starting to get bothersome. Cervix measures 1 finger tip (Technical term huh!?)
March 5th 2004 - 3pm - Pletocin is given to induce labor
March 5th 2004 - 11am - Immediately we go down to the hospital with the same routing expected to follow. And it didn't. Her blood pressure remained high, her proteins now measure 1+ at the hospital. It was now time to induce.
March 5th 2004 - 7am - Again we go in for a checkup with our regular doctor at our regular clinic. They cannot figure out why the hospital found very little of anything, while the clinic found so much. Again they ran the urine to check, and were about to draw blood when the test came back 2+.
February 28-29th 2004 - LAMAZ CLASS at the very same place we were the day before. Very informative, but now was old hat except for the breathing part. But we did pass!!
February 27th 2004 - Another scheduled doctors visit as we are now approaching 37 weeks, and have weekly visits with our care giver. The doctor received the results of the blood work, and asked Rachel to supply her usual urine sample, and expedited a protein test on it. She showed 1+ for proteins If you don't know, if you have 2+ proteins they hospitalize you due to the very good possibility that your kidneys are shutting down. And her platelets were too low, then add the swelling and headaches, with high blood pressure,which all lead to a problem. So they pointed us to the door and said your hospital bound!! After calling grandma to hang onto Kjerste, running by home real quick to grab a car seat and a suitcase, we headed to Mercy hospital in Coon Rapids, MN. Upon arrival they registered Rachel quickly, got an arm band and we headed to the birthing center. They hooked her up to a couple machines and watched her, after getting their own samples. After about 5 hours all the labs had come back and the doctor talked to us and prescribed complete bed rest. The platelets came back normal, and they only found a trace of protein in her urine. Her blood pressure had been a problem all along, and now with the excitement was VERY high, but with rest, and fluids, it came down, and so did the swelling. We asked about the Lamaze class we were to take that weekend and we got the OK for that, but nothing else.
February 25th 2004 - received a call from the clinic asking Rachel to come back in and give a blood sample, and another urine. sample. Seems there were traces of protein in her urine. and it usually indicates preclamcia. She proceeded to the clinic for the blood to be drawn.
February 20th 2004 - our house awoke as normal, Kjerste was headed to grandma's house while Rachel and I prepped for a scheduled doctors visit at the local clinic. Upon arrival she was handed a label and a cup, and directed to go to the little girls room. This is normal procedure for anyone that is pregnant, just ask them. We had a basic checkup, and everything looked ok. Rachel was swelling in the feet (not abnormal either, just ask a pregnant person) and legs, and was directed to take it easy, drink plenty of fluids, and try to get her feet up a couple hours during the day.
The Beginning- Starting at the bottom
Links of Kyle |
|||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}